English
English Français
Français Español
Español Português
Português عربى
عربى 日本語
日本語 한국어
한국어
Silicone Foam Dressings: A Buyer’s Guide for Hospitals and Distributors
Content
- 1 What Are Silicone Foam Dressings and How Do They Work?
- 2 Key Clinical Benefits: Evidence‑Based Advantages
- 3 Silicone Foam Dressing Selection Matrix: Exudate Level, Wound Location, and Budget
- 4 Cost Analysis: Why Bulk Procurement of Silicone Foam Dressings Saves Money
- 5 Top Brands Compared: Dimora, NoTraum, McKesson, and More
- 6 Customization and OEM Options for Bulk Buyers
- 7 How to Order Silicone Foam Dressings in Bulk from Texnet
What Are Silicone Foam Dressings and How Do They Work?
A 200‑bed hospital goes through roughly 12,000 wound dressing changes each year. The wrong choice can mean excruciating removal pain, macerated periwound skin, and nursing shifts lost to frequent re‑dressing. Silicone foam dressings are designed to solve exactly that trio of problems.
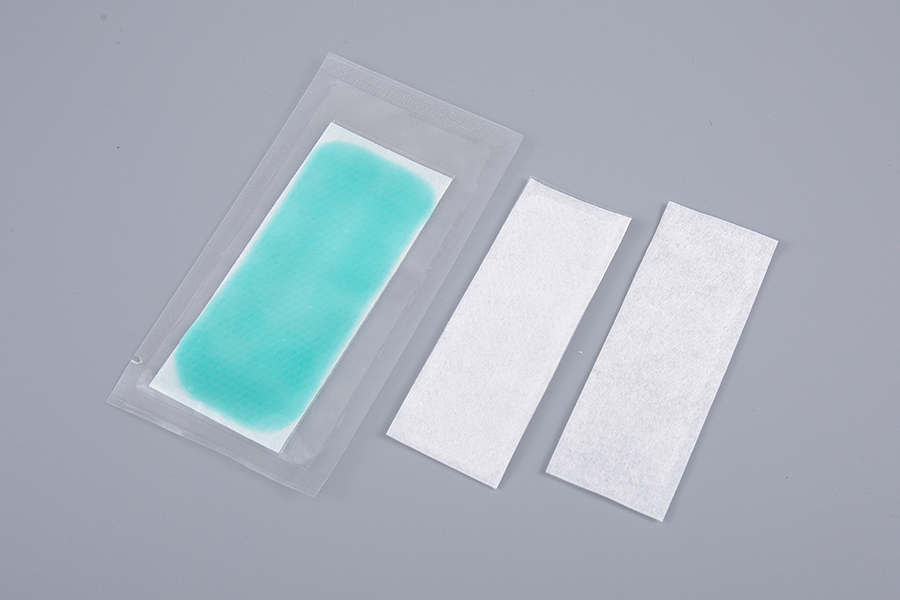
These dressings consist of five distinct layers. The outermost backing film repels fluids and bacteria while letting oxygen pass. Just beneath it, a super‑absorbent polyurethane foam core locks exudate inside—often up to 15 times its own weight. A perforated silicone gel adhesive layer contacts the skin, providing a secure seal that doesn’t bond to the moist wound bed itself. Between the foam and silicone sits a non‑adherent wound contact layer that wicks fluid one way, away from the skin. Finally, a polyethylene or polypropylene release liner protects the adhesive until application.
The clinical logic is straightforward: keep the wound bed moist but the surrounding skin dry. That balance speeds epithelialization and slashes the risk of maceration. Because the silicone adhesive attaches only to dry, intact skin, removal causes 60 % less pain and virtually no epidermal stripping compared with traditional acrylic adhesives.
Key Clinical Benefits: Evidence‑Based Advantages
Pressure injuries add an estimated $10.7 billion to U.S. healthcare costs annually, yet the 2019 NPUAP/EPUAP guideline clearly states silicone foam dressings can prevent them. For sacral and heel sites the recommendation carries an Evidence Level A—the strongest possible—when the dressing is applied prophylactically to intact skin.
Beyond prevention, the data tell a consistent story. A 2021 meta‑analysis of 14 randomized trials found silicone foam dressings reduced pressure‑injury incidence by 58 % compared with standard non‑foam regimens. Separate studies measuring pain during dressing changes reported a mean VAS score drop from 4.7 to 1.8 when switching from traditional gauze to silicone foam. The same analysis noted a 40 % reduction in periwound maceration, a direct result of the dressings’ high moisture‑vapor transmission rate (often above 2,000 g/m²/24 h) coupled with vertical wicking.
The infection picture also shifts. By maintaining a closed, moist environment and avoiding adhesion‑related skin tears, silicone foam dressings cut secondary wound infections by roughly one‑third in published post‑surgical studies. Those numbers matter when evaluating total cost of care.
| Metric | Silicone Foam | Hydrocolloid | Cotton Gauze |
|---|---|---|---|
| Pressure‑injury prevention (Evidence Level) | A (NPUAP/EPUAP) | B | Not recommended |
| Pain on removal (VAS 0‑10) | 1.8 | 3.2 | 4.7 |
| Maceration rate | 8 % | 22 % | 31 % |
| Average wear time (days) | 3–7 | 2–4 | ≤1 |
Silicone Foam Dressing Selection Matrix: Exudate Level, Wound Location, and Budget
Procurement teams rarely face a one‑size‑fits‑all scenario. The right dressing depends on three hard variables: exudate volume, anatomical site, and available per‑unit budget. The matrix below maps those variables to product specifications that drive performance—namely foam thickness, shape, and backing properties.
| Exudate / Site | Low Exudate (mild serous) | Medium Exudate (serosanguinous) | Heavy Exudate (frank fluid) |
|---|---|---|---|
| Sacral / Coccyx | 4 mm foam, 15×15 cm square, economy tier ~$2.20/unit | 6 mm foam, 15×20 cm butterfly shape, standard tier ~$3.10/unit | 8 mm super‑absorbent, 15×20 cm butterfly, premium ~$4.50/unit |
| Heel / Ankle | 4 mm, 10×10 cm U‑shape, ~$1.80/unit | 6 mm, 12×12 cm U‑shape, ~$2.60/unit | 8 mm, 13×13 cm U‑shape with extra pad, ~$3.90/unit |
| Tracheostomy | 4 mm, 8×8 cm split‑flange, ~$1.50/unit | 6 mm, 9×9 cm split‑flange, ~$2.00/unit | Not recommended–use foam with antimicrobial layer |
Heel and sacral sites demand shapes that offload shear force. Butterfly‑cut sacral dressings let the adhesive wings stretch laterally while the foam pad stays centered over the bony prominence. U‑shaped heel dressings wrap the posterior curve without creating bulk that shifts inside footwear. Tracheostomy dressings with a pre‑cut split flange slide around the tube and seal with minimal manipulation.
For moderate‑to‑heavy exudate, look for a minimum foam thickness of 6 mm and a vertical‑wicking layer. Budget‑conscious bulk buyers can often opt for economy lines with 4 mm foam on low‑exudate wounds and still achieve 3‑day wear times. When placing large‑volume orders, specifying SKUs by thickness‑shape‑sterility speeds up warehouse slotting and clinical uptake. The silicone tape used for secondary fixation should match the dressing’s adhesive profile—gentle removal is the whole reason to standardize on silicone.

Cost Analysis: Why Bulk Procurement of Silicone Foam Dressings Saves Money
The unit price of a silicone foam dressing is higher than a gauze square, but that view misses two‑thirds of the real cost. Nursing time, sterile supplies for re‑packing, and complication treatment together consume far more budget than the dressing itself.
Model a 200‑bed acute‑care facility with an average daily census of 30 stage‑II or worse wounds. Under a gauze‑based protocol, nursing staff change dressings 2–3 times daily, spending 12 minutes per change including hand hygiene, PPE donning, and documentation. That translates to roughly 21,900 nurse‑minutes per year—365 hours. At a fully loaded labor cost of $45 per hour, the annual nursing bill for gauze‑dressing changes sits around $16,425.
Switching to silicone foam with a 5‑day wear time drops dressing changes to about 2,190 annually. Even at a conservative 10 minutes per change, the nursing hours shrink to 365 total, costing $16,425 per year for labor. Stay with the numbers: gauze protocol also demands a new sterile tray, saline, and secondary wrap each change, adding $1.80 in ancillary supplies. Silicone foam eliminates those ancillaries because the border acts as a secure secondary cover. Factoring both labor and ancillaries, the total annual wound‑care cost for our 200‑bed hospital runs $38,000 with gauze versus $23,000 with silicone foam—a $15,000 saving, despite a higher per‑dressing purchase price.
| Cost Category | Gauze Protocol | Silicone Foam Protocol |
|---|---|---|
| Dressing changes per year | 21,900 | 2,190 |
| Nurse hours | 4,380 | 365 |
| Labor cost ($45/h) | $16,425 | $16,425 |
| Ancillary supplies per change | $1.80 | $0.00 |
| Total annual cost | $38,000 | $23,000 |
Bulk procurement contracts that lock in pricing across 12‑month periods let materials managers treat silicone foam as a predictable line item. When combined with a procedure kit dressing strategy that bundles foam, tape, and gloves into a single SKU, inventory turns improve and wastage drops further.

Top Brands Compared: Dimora, NoTraum, McKesson, and More
Hospital buyers often split their formulary between two or three manufacturers to balance performance and price. The table below captures the specifications that matter most to value‑analysis committees: absorption capacity, border adhesion strength, size range, and typical U.S. bulk price per unit.
| Brand | Absorption (mL/100 cm²) | Border Adhesion (N/cm) | Common Sizes (cm) | Bulk Price (per unit, ≈) |
|---|---|---|---|---|
| Dimora | 2,800 | 2.2 | 10×10, 10×20, 15×15 | $2.10–$4.00 |
| NoTraum | 3,100 | 2.8 | 10×10, 10×20, 15×20 | $2.50–$4.70 |
| McKesson | 2,900 | 2.4 | 10×10, 10×20, 15×15, 20×20 | $2.30–$4.20 |
| ActivHeal | 2,600 | 2.0 | 10×10, 10×20, 15×15 | $1.90–$3.50 |
| Texnet Private‑Label | 2,750–3,200 | 2.3–3.0 | Custom from 10×10 to 20×20 | MOQ‑based, from $1.70 |
NoTraum leads on outright fluid capacity, which makes it a frequent pick in burn units and high‑exudate wounds. Dimora and McKesson balance price with reliable adhesion, dominating med‑surg floors. ActivHeal offers a budget‑entry alternative without sacrificing the core silicone‑gel layer. Texnet’s private‑label line bridges the gap by letting buyers specify absorption grade and border adhesion within a single contract, ideal for health systems that want formulary consistency across facilities.
Customization and OEM Options for Bulk Buyers
Standard catalogs rarely fit every contractual requirement. Large hospital networks and distributors often need private‑brand packaging, a sterile single‑pack format, or a particular shade of blue that matches their existing kit aesthetics. OEM‑capable manufacturers like Texnet offer a structured menu of customizations that turn a commodity into a system‑aligned product.
- Absorption grade: from 4 mm standard to 8 mm super‑absorbent foam core, selectable per SKU.
- Adhesive strength: soft‑touch silicone at 2.0 N/cm for fragile skin up to 3.0 N/cm for active patients.
- Shape: standard square, butterfly, U‑shape, split‑flange tracheostomy, or die‑cut to your template.
- Sterile packaging: single‑unit peel pouch or multi‑unit tray with custom printing and barcoding.
- Color: backing film in white, blue, or custom Pantone‑matched shade.
- X‑ray detectable line: included or omitted based on cost preference.
Minimum order quantities typically start at 10,000 units per SKU for shape‑adhesive‑color combos. Lead times run 45–60 days for initial production, with a 30‑day re‑order cycle once tooling and validations are complete. Asking for a pilot batch of 500 units is a low‑risk way to test clinical acceptance before committing to a full production run.
How to Order Silicone Foam Dressings in Bulk from Texnet
Starting a bulk procurement conversation is simpler than running a comparative trial. Texnet invites hospitals, distributors, and group purchasing organizations to request a product dossier that includes absorption test reports, adhesion peel‑force curves, and sterility assurance documentation. That data package allows materials managers to evaluate silicone foam dressings against current contracted products without waiting for physical samples.
Send a detailed inquiry specifying annual volume, preferred sizes, and any OEM requirements. The sales engineering team responds within one business day with a matched proposal that covers pricing tiers, MOQ exceptions for pilot orders, and logistics options. Trade‑show attendees can also schedule a meeting at the next FIME Miami event to see the latest silicone foam prototypes and test the adhesion firsthand. For teams already sourcing surgery and nursing supplies, consolidating silicone foam dressings into an existing vendor relationship slashes administrative overhead and unlocks volume‑discount thresholds.